| This is a Draft Amnesty Week draft. It may not be polished, up to my usual standards, fully thought through, or fully fact-checked. |
| Commenting and feedback guidelines: This draft lacks the polish of a full post, but the content is almost there. The kind of constructive feedback you would normally put on a Forum post is very welcome. |
Summary
- Most global health charities and evaluations focus on metrics that only focus on post-birth outcomes, such as Lives Saved or DALYs (Disability-Adjusted Life Years)
- But it can be argued (according to plausible assumptions) that birth is an arbitrary dividing line, and that unborn children and/or potential lives also have moral worth
- Whether we choose to model birth as the most important dividing line or not has a significant impact on how effective certain charitable interventions are
- I divide worldviews into a simplified "pro-life" person-affecting worldview (early life has moral worth, foetuses count as people) and a simplified "pronatalist" non-person-affecting worldview (the more humans, the better, regardless of whether they "exist" yet). I also consider an anti-natalist worldview (life has negative moral value) briefly for comparison.
- I focus on global health interventions that can be robustly good considering according to both mainstream and pro-life/pronatalist perspectives, and find that:
- If unborn lives are given moral weight, many mainstream interventions - malaria prevention/treatment in pregnancy, syphilis screening and antibiotic treatment, and micronutrient supplementation - become substantially more cost-effective than standard DALY models suggest.
- A few other options, like infertility prevention through schistosomiasis control and STI screening, could be especially promising from a pronatalist perspective.
- From an moderately anti-natalist or suffering-focused perspective, we should probably prioritise WELLBY-focused charities
- I propose that most interventions framed as "pro-life" are probably far less effective than these global health charities, regardless of your stance on when moral value begins
Overview Table
| Worldview | Moral premise | Example interventions / areas | Speculative recommended charities |
|---|---|---|---|
| A. Person-Affecting (Foetuses are people) | Moral value begins before birth; preventing foetal loss counts like saving an existing life | Malaria prevention in pregnancy (ITNs, IPTp-SP); syphilis screening & treatment; micronutrient supplementation; MgSO₄ for pre-eclampsia | Against Malaria Foundation, Malaria Consortium, Healthy Futures (syphilis screening), Helen Keller International (micronutrients), Population Council (IPTp-SP initiatives) |
| B. Non-Person-Affecting (All potential lives matter) | Creating new happy lives adds moral value; infertility prevention generates moral benefit | STI screening/treatment (chlamydia, gonorrhoea, syphilis); schistosomiasis control (praziquantel); post-abortion infection care | Pilot STI-screening projects (e.g., Healthy Futures); Unlimit Health (schistosomiasis treatment) |
| C. Anti-Natalist / Suffering-Focused | Human life has neutral or negative expected value; focus on reducing suffering without increasing births | WELLBY-oriented interventions; malaria chemoprevention; mental-health and pain-reduction initiatives | WELLBY-focused charities (e.g. Pure Earth; Taimaka); Malaria Consortium (chemoprevention) |
Intro
I was recently reading Ozy Brennan's monthly EA updates (linking to a Vox article):
In areas where malaria is endemic, malaria may be responsible for as many as a quarter of all maternal deaths. Women with malaria infections are three to four times more likely to miscarry, as well as being more likely to experience stillbirth. I highly recommend the Against Malaria Foundation for all pro-life donors; if you think foetuses are people, it’s by far the best way to turn dollars into lives saved.
I couldn't find the reasoning for the idea that AMF is "by far the best way to save lives". Sure, it's plausible, given that AMF is already really effective, but surely we need to run the analysis!
So I set to asking the question: What are the most effective charities for saving human lives, given worldviews where life obtains moral value at an earlier stage?
Why research this?
There's often a bit of confusion with the metrics we use to measure global health, seeing as people have very different priors on what counts as a life and how to value it.
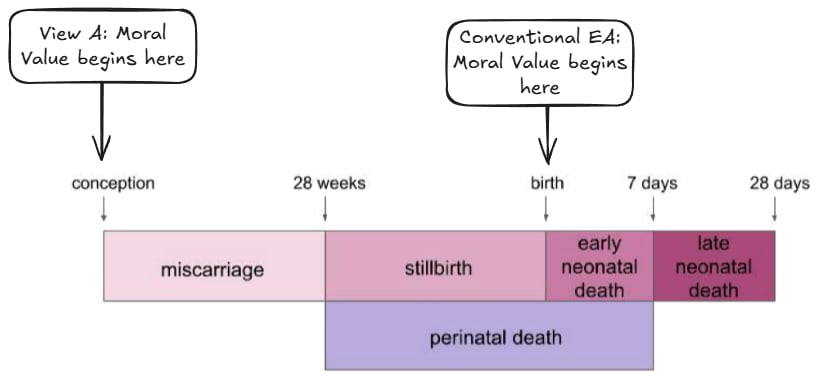
As far as I understand, in standard global health accounting, miscarriages and stillbirths are ignored, while the death of a live-born infant counts as roughly 70 DALYs lost.
This should strike you as slightly odd.
By contrast, slightly more "pro-life" worldviews would allocate the DALY value of pre-natal deaths more similarly to deaths of live-born infants. This seems relatively reasonable given certain not-crazy priors:
- Human lives are generally worth living;
- Saving a potential life produces a similar amount of positive value as saving an current life, adjusting for the negative value associated with death.
So my bottom line is that a system that assigns unborn foetuses the same moral value as new-borns seems to me about as rational as the mainstream global health framework, where moral value begins at birth, and preventing a death is good, while creating a life is morally neutral.
When evaluating charities, I think it's super important to think about how moral assumptions about when life gains value might shift our priorities. Given moral uncertainty, it's especially important to recognise when many interventions remain robustly effective across worldviews, and others don't.
So I think it's worth asking: should our recommended charities change under two broad secular pro-life or pronatalist assumptions?
- Pro-life: a person-affecting view where foetuses already count as people, so preventing miscarriage or abortion is morally equivalent to saving an existing life
- Pronatalist: a non-person-affecting view where creating new, happy lives is itself good, even if those people don’t yet exist
I also look at anti-natalist angles at the end for comparison.
View A: Early life has moral worth; foetuses count as people
From a secular perspective, if life begins in pregnancy, we can value an unborn baby as: a) a potential human being who can experience all of the potential upsides and downsides of life; and b) already sentient/human enough to be worthy of moral consideration. This perspective is also "person-affecting", so it is much more important to save the life of an unborn child than to create a new child from scratch.
If you believe that we should draw a relatively hard line of moral worth after conception and before birth, you should weight your charity-effectiveness calculations towards charities that help currently existing foetuses to be born.
To work out how to do this, there's a few questions we need to answer:
- Are pregnancy losses comparable in number to child deaths?
- What are the main causes of pregnancy loss?
- What are the most cost-effective solutions we have?
Pregnancy Loss Numbers & Causes
Firstly, pregnancy loss globally massively outweighs neonatal death. There are around 73 million abortions a year, compared to about 2 million reported stillbirths (late stage pregnancy loss) every year - mostly in poor countries, and an estimated 23 million miscarriages. This compares to 4.8 million deaths of children under 5, meaning that about 95% of deaths post-conception are prenatal.
There's a methodological issue where basically no-one reports or investigates early-stage pregnancy loss, especially in poor countries, but I'd give the following (very rough) estimate of causes for miscarriage and stillbirth from what I could find:
- Chromosomal or genetic anomalies: 40-60% of all pregnancy loss, most common in earlier stages (source)
- Infections: 15-25% (malaria, syphilis, toxoplasmosis, HIV, Listeria) (source); very common in later stages
- Maternal malnutrition or anaemia: 5-15% (guess based on this source) - infections can also interact with malnutrition or anaemia
- Hypertensive disorders (pre-eclampsia): 5-10%, mostly late-stage (source)
- Obstetric complications: maybe 5-15%? Hard to disentangle from other causes.
- Others: <5% (e.g. physical harm to the mother)
We don't need to dive into the data too much to narrow down which of these are the most tractable. Chromosomal anomalies are clearly not tractable, so scratch that. Obstetric complications are probably tied to general health system strengthening, and difficult to isolate with a single intervention or charity. Infections, maternal nutrition and hypertensive disorders seem worth looking into. Fortunately, we have data on maternal outcomes from these, so we can extrapolate how many potential lives are lost here.
Hypertensive Disorders
According to the WHO’s Trends in Maternal Mortality report, hypertensive disorders such as (pre-)eclampsia are one of the major causes of both maternal death and late-term stillbirth. Abnormal development of the placenta can cause high blood pressure (pre-eclampsia), which may lead to seizures and organ failure, which risk killing both mother and baby.
We have a miracle fix in the form of magnesium sulphate (MgSO₄) treatment, which prevents these seizures by calming the nervous system and stabilising nerve activity. It's under a dollar per person to provide, and incredibly effective.
But sadly, like so much in global health, it seems that the binding constraint is not usually the delivery of MgSO₄, but things like screening and delivery services. I couldn't find any listed effective charities that focused on this, so this is unlikely to be tractable with donations.
The verdict: Probably not the most promising, but worth paying attention to.
Maternal malnutrition and anaemia
Poor maternal nutrition, in particular, iron-deficiency anaemia, seriously affects pregnant women and unborn babies. According to the WHO, around 35% of pregnant women globally are anaemic, most due to dietary iron deficiency, but often worsened by infections (see below). Anaemia increases the risk of miscarriage, stillbirth, and maternal death, mainly because reduced oxygen transport stresses both the mother’s heart and the developing foetus.
Unlike hypertensive disorders, I identified some effectiveness-oriented charities working on this! There are a bunch of focused charities that provide malnutrition treatment and iron supplementation, or multiple micronutrient supplementation (MMS), in neglected regions. Charities with some support from EA funders, like Helen Keller International, the Eleanor Crook Foundation and World Vision, provide targeted programs for pregnant women.
A relatively recent review (Engle-Stone et al, 2019) estimated that, in areas already receiving iron supplementation, switching from iron–folic acid (IFA) supplements (the standard treatment) to multiple micronutrient supplements (MMS) for pregnant women could avert a child's death for $125–$180 per life saved. This paper is a rare exception that counts stillbirths, as well as infant deaths. The authors did not include early miscarriages, but adding these to the equation could make the intervention even more effective.
It seems very scalable too. ECF says:
"MMS costs less than $0.02 per tablet – or $4 per pregnancy. For a total of $1.1 billion, we could reach 260 million women with MMS by the end of 2030."
The verdict: Needs more serious research, but, seeing as there are already highly-effective organisations working in this space and room for huge expansion, providing micronutrient supplements is likely to be even more effective from a "pro-life" angle.
Infections (other than malaria)
Infections while pregnant are a massive risk. Although any infection can harm both mother and baby, malaria and syphilis seem to be the worst. Some other infection-related causes of stillbirth are listed in this article: e.g. toxoplasmosis, cytomegalovirus, listeria, rubella, parvovirus B19, and Zika. These are mostly pretty sporadic, therefore there probably won't be scalable interventions.
Syphilis is pretty devastating. It's responsible for an estimated 150,000 miscarriages / stillbirths and 70,000 neonatal deaths each year. Interventions are simple and effective: a single injection of benzathine penicillin during pregnancy prevents nearly all congenital infections, and relatively low-cost behavioural interventions can limit transmission.
A WHO-funded modelling study by Kahn et al. (2014) found that scaling up antenatal syphilis screening and treatment could avert between 5,700 and 93,000 DALYs per million pregnancies, with a cost-effectiveness of roughly $24–$111 per DALY. That study used a conservative assumption that a stillbirth represents about 4.9 DALYs lost. If we apply a logic where a stillbirth has similar value to an adult child, the cost-effectiveness starts looking more like $2-10 per DALY!
Unlike malaria, syphilis doesn't have such a strong infrastructure of effectiveness-focused organisations working on implementing the most effective interventions, but Evidence Action (recommended by a Life You Can Save), is running maternal syphilis programmes. Healthy Futures, a Charity Entrepreneurship funded organisation, is also carrying the EA flag here! They're working with the Department of Health in the Philippines to design a pilot of dual HIV/syphilis testing for pregnant women. Expect exciting things!
The verdict: Weighting unborn lives similarly to children, syphilis interventions could jump to becoming a top charity!
Malaria
As well as being horrible in lots of ways, Malaria is also major cause of miscarriage, stillbirth, and early neonatal death. In high-transmission regions, most adults have acquired partial immunity, so malaria infections are a bit like getting the flu. But pregnancy screws up your immunity, making women, especially in their first or second pregnancies, vulnerable again. Even if many malaria infections in pregnancy are asymptomatic or mildly symptomatic, they can still lead to anaemia (see above) and infect the placenta.
Reports estimate that roughly 12–13 million (36%) pregnancies are exposed to malaria. The consequences are bad: placental infection can starve the foetus of oxygen, increase stillbirth and preterm birth risk, and contribute to chronic undernutrition in surviving infants. A paper estimated that 8% of stillbirths globally were associated with malaria - similar to those associated with syphilis.
So, AMF?
The currently recommended malarial interventions per GiveWell are:
| Intervention | Cost per life saved (GiveWell) | Lives included | Notes |
|---|---|---|---|
| Seasonal Malaria Chemoprevention (SMC) – Malaria Consortium | $4,000 | Children under 5 only | Prevents child deaths in high-transmission months. |
| Insecticide-treated bed nets (ITNs) – Against Malaria Foundation | $5,500 | Children under 5 only | Life-saving estimates exclude fetal losses. |
If you rate the lives of unborn children equally, then ITNs probably wins out, because providers also recommend that pregnant women sleep under bed nets, but, at least according to GiveWell, SMC doesn't extend to pregnant women. A Cochrane review found that ITN use by pregnant women reduced placental malaria by ~38% and maternal anaemia by ~23% in first or second pregnancies. Because malaria in pregnancy accounts for a large share of stillbirths and neonatal deaths, and ITNs substantially reduce placental malaria, including these effects could increase the estimated impact of bed nets by around half again.
So your favourite charities may have become even more effective!
But AMF might not actually win out here, as there are more targeted interventions that specifically target pregnant women.
Intermittent preventive treatment with Sulphadoxine-Pyrimethamine (IPTp-SP) for pregnant women seems to be more cost-effective than bed-nets for preventing malaria-related neo-natal deaths and stillbirth/miscarriage. A 2023 BMJ Global Health analysis estimated a cost of $33–$80 per DALY averted, even when counting only neonatal deaths and harms to the mother, not stillbirths or miscarriages. At a guess, with prenatal deaths included at similar rates, the true cost per DALY could plausibly drop by 3x or 4x. Similar to syphilis, the raw numbers (under $20 per DALY averted) start looking incredibly good here.
But, unlike bed-nets or chemoprevention, there doesn’t seem to be a charity that exclusively provides IPTp-SP for pregnant women. Groups like the Population Council are working on it, but I think it's mostly funded as part of general antenatal care, which you can't support directly.
The verdict: A relatively confident recommendation here is: if you lean "pro-life" you should choose bed-net charities over chemoprevention for children. If there is an intervention or charity that's able to effectively get IPTp-SP to pregnant women in a targeted way, it might be even better than bed-nets. It seems that donating to charities that provide holistic care to new mums including IPTp-SP might be a good bet, but I couldn't identify a way of focusing donations for that.
Abortion and explicitly "pro-life" charities
There are two controversial (many votes, positive and negative) EA Forum posts on this topic (Ariel's and Calum's). As mentioned earlier, the scale of abortions is significantly higher than stillbirths, miscarriages and neonatal deaths put together. While I'm sure none of my readers are keen on relitigating the abortion debate here, it's important to at least think about these comparisons.
While there are obvious downsides to any charity or intervention with the aim of reducing abortions, supporting/nudging pregnant women to carry their babies to term when abortion is a possibility is likely to be a relatively low-cost way of bringing new life into the world. Also, as abortion reduction can produce new babies in rich countries, where they're more likely to have a net-positive life, there might be other utilitarian arguments for such an approach.
So is there a better option here?
There's a bunch of Christian "pro-life" charities that support young women to bring their pregnancies to term, often when they are considering an abortion.
Regardless of whether this aligns with your morals, are they effective?
No idea.
Unlike the global-health sector, where interventions are evaluated in randomised trials and reported in DALYs, most “pro-life” charities collect almost no reliable data. As far as I can tell, basically none disclose how many women they reach, what proportion would otherwise have had abortions, or other important data such as the long-term wellbeing of the mothers and children.
Forgive my cynicism here, but because of the incentives in this kind of religious donor landscape, my guess is that very few of these charities provide this kind of care cost-effectively.
As the previous post mentions, there are also legislative efforts to adjust laws around abortion. As well as banning abortion, this could involve more palatable approaches, such as adjusting the gestational age limits in countries which allow later stage abortions. I couldn't get any good cost-effectiveness estimates, but I would be surprised if legislative interventions in countries with intense, highly-funded debates on the topic could reach the effectiveness of the global health charities mentioned above.
This is mostly speculation, though, and I'm curious what a steel-manned version of this argument would look like.
View B: More people = better world; potential lives are intrinsically valuable
This "human maximisation" worldview assumes a net-positive future where the marginal human doesn't make the world bad in other ways (e.g. animal welfare), and where we would want as many happy humans on earth as possible.
According to this view, a painless death of a child can be seen as morally equal to preventing a birth through contraception, abortion, or miscarriage. Similarly, saving an existing child is also morally similar to incentivising a new birth.
This would surely really change our calculations.
So are there incredibly cheap ways of ensuring that more children are born?
I actually wrote a Substack post on effective spending to increase global birth rates (please subscribe if you enjoy), but this was mainly focused as a narrow response to "paying people to have babies" arguments. The (very casually modelled) conclusion is that we should prioritise countries that are poor, but have high birth rates, education levels and well-being ratings (Central Asia wins out). I found no current charities working on this.
But there might be better approaches. If you're purely maximising for the number of people born, and you don't care so much about education and happiness, you should probably look at ways of allowing the poorest women to have more children. The lowest-hanging fruit here looks like protecting fertility in places where people already want more children but can’t have them. There seem to be three pretty good ideas here:
STI screening and treatment (chlamydia, gonorrhoea, syphilis)
Roughly 3–4% of women globally have active chlamydia, and about 20–25% of untreated cases progress to pelvic inflammatory disease (PID), which causes infertility in roughly one-fifth of cases. Treating 1,000 infected women therefore prevents about 30 cases of infertility.
At the intervention level, this looks cheap. At around $15 per woman for testing and antibiotics, that’s roughly $500 per infertility case prevented, or $700–800 per additional life created (assuming 60–70% go on to give birth). Add gonorrhoea and syphilis to the mix (which can be screened for together), and this could get even more effective.
The Gates Foundation recently committed $2.5 billion towards improving reproductive and maternal health technologies in low-resource settings, suggesting the broader global health community takes this area seriously. However, I couldn't find very targeted NGOs working on this.
The verdict: Seems robustly good as a pro-natalist cause area, but no clear charity options.
Schistosomiasis control
Urogenital schistosomiasis affects around 100 million women worldwide and can cause infertility by scarring reproductive tissue. Mass treatment with praziquantel, usually delivered through national “deworming” campaigns alongside other antiparasitic drugs, costs just $0.30–$0.50 per person per year.
Although I couldn't find trials quantifying how much praziquantel prevents infertility, there’s clear evidence that the relationship is non-zero. Women in high-prevalence areas of Schistosoma haematobium infection have 20–50% higher odds of infertility than those in low-prevalence areas (Woodall & Kramer 2018). This strongly implies that treatment and prevention programmes would protect fertility.
Given the raw costs, if it prevents infertility in even 0.5% of women treated, that’s around $100 per infertility case prevented, or <$200 per life created. This is already supported by major evaluators such as GiveWell and The Life You Can Save through organisations like Unlimit Health (formerly SCI Foundation).
The verdict: This could be a great way we have of increasingly global fertility among people who want to have children! Even if the most recent papers have massive uncertainty as to the impacts, Unlimit Health seems a robustly good choice for the pronatalist donor.
Safe delivery and post-abortion care
Around 7 million women each year suffer complications from unsafe abortion; and many develop infertility, mostly in Sub-Saharan Africa. A recent study found in the DR Congo that ~43.3% of women with secondary infertility had a history of unsafe abortion.
This seems tractable. Post-abortion care, typically antibiotics and uterine evacuation, costs around $20–40 per case. A very naive estimate assuming that 1) around 10% of untreated complications lead to infertility, 2) timely treatment prevents 90% of these cases, and 3) roughly 60–70% of women whose fertility is preserved will go on to have a child, the cost works out to about $200–400 per infertility case prevented, or $300–600 per additional birth made possible.
Quite a lot of organisations work on these issues, like IPAS and Marie Stokes International. It's kinda interesting that organisations supporting or providing safe abortions may actually have a positive impact on lifetime fertility in some cases, but the fact that the same orgs provide the abortion and the post-abortion care means that it's hard to recommend purely from a pronatalist perspective.
The verdict: I couldn't find good enough data, or targeted organisations, to make decent estimates here. Could potentially be a promising "common ground" for people with pro-life or pronatal, and pro-choice positions.
View C... What if you're anti-natalist?
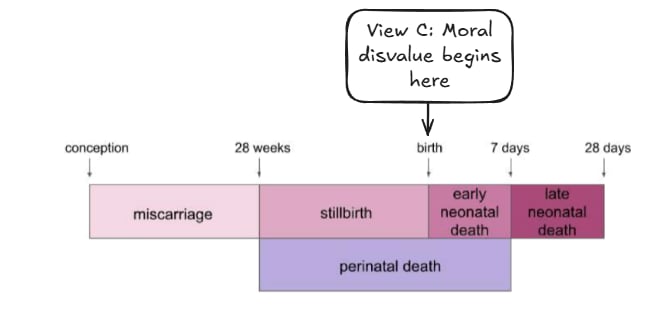
For the anti-natalist, I also think there are reasonable arguments for a perfect mirror-image of the pronatalist arguments I've made here!
If you think that a significant proportion of human life is net-negative value, or that harms to farmed animals mean that we should be trying to reduce human population, at least until we stop factory farming, it's perfectly reasonable to downgrade the cause areas/charities described in the article.
In this case, please reverse all the recommendations above!
If you still want to focus on saving human lives, without producing new lives, then malaria chemoprevention seems better than bed-nets. Family-planning focused charities might also be a better bet, especially those working in areas with very high fertility.
Finally, I strongly recommend the work of the Happier Lives Institute, if you want to focus on human-focused charities that focus on well-being and suffering reduction, rather than those that focus purely on saving lives, regardless of the quality of those lives.
Conclusion
Hopefully this should give people with different worldviews a clearer idea of what global health charities would be more appropriate for them to support.
Writing this was pretty interesting for me. It's very rough with the figures, so I welcome more careful analysis of these arguments!
- ^
Obviously this term is annoying, but I can't think of a better, more concise term for the moment
- ^
I also know that many people who believe in pro-life causes also believe in doctrinal Christianity, which tends to include belief in Heaven and Hell (infinite pleasure vs. infinite suffering). Given the infinite value at stake, they should definitely be prioritising making sure no-one goes to Hell!
Thanks for writing this - I'm a pro-life EA, which feels like being a member of a rare species, and so I appreciated you posting this here. I thought the diagrams were an especially nice touch!
Great post, Zack! Strongly upvoted.
It costs AMF 2.67 k$ (= 2/3*4*10^3) to increase population by 1 if you are right this cost is 2/3 (= 1/(1 + 0.5)) of its cost to save a life. That is 3.12 (= 2.67*10^3/855) times GiveWell's estimate for the cost to save a life via dietary salt modification, and GiveWell identified Resolve to Save Lives (RSL) as a promising charity that could absorb funding to implement this. So I am thinking RSL is one of the most cost-effective ways to increase human-years.
Hi Jack,
thanks for putting together and sharing this piece.
That said, I found one aspect important to flag:
This makes the piece feel one-sided: it quantifies the value of potential lives but abstracts away the people who bear the physical and ethical burden of bringing those lives into existence.
I’m sharing this as constructive feedback. I think the analysis could be stronger and more balanced if it explicitly integrated maternal health outcomes and the ethics of pregnancy itself, not only the unborn.
Hi Klara, thanks for the response.
I don't think I am entering the abortion debate by assigning moral value to unborn lives any more than I'm entering any other debate that considers unborn or potential lives (e.g. the ethics of moderate drinking while pregnant, the ethics of having children in space, or the repugnant conclusion).
I think I'm comfortable with having mostly sidestepped the maternal health issues, given that I was focusing on interventions that are robustly good for the mother. If I were to do a stronger and more robust cost-effectiveness analysis, or tackle more controversial interventions where the interests of the mother and child clearly diverged, I would consider maternal health outcomes separately. I hope my piece makes it clear that we should prioritise uncontroversial and neglected interventions that treat or prevent painful conditions that women suffer from.
Although I do recognise that the ethics of pregnancy, lived experience of the mother, and autonomy trade-offs are important considerations, I'm afraid that attempting to tackle these here would have made this an impossibly long post!
I know some that plausibly save tens or hundreds of thousands of lives a year on a very low budget, but they are quite low-key so it is hard to say more.
What sorts of things do they do?